Diagnosed With Advanced Colorectal Cancer, Young UK Researcher Fights Back
LEXINGTON, Ky. (June 24, 2021) — Early in the evening of May 30, 2020, UK HealthCare trauma surgeon Dr. Zachary Warriner prepared an emergency operation to figure out the cause of a bowel obstruction. His patient, a 27-year old man, had come into the emergency department earlier that day with the vague symptoms of severe belly pain and nausea.
“He was in pretty significant discomfort,” said Warriner, assistant professor in the University of Kentucky College of Medicine Department of Surgery. “He was miserable and looking for some kind of relief.”
When a CT scan confirmed the blockage, Warriner’s team first tried a less invasive approach, attempting to use a colonoscope to pass the blockage and alleviate the pressure in his intestines. After attempting the procedure with various scopes to no avail, the surgery team had no choice but to open him up for an exploratory laparotomy to see exactly what was going on.
Around 1 in the morning, Warriner contacted the pathologist on call with bad news: he needed a tumor biopsy.
This young patient, who had no family history of cancer, was diagnosed with a worst-case scenario: advanced colorectal cancer that had eroded through the wall of his colon and had spread to the lining of his abdominal cavity.
*****
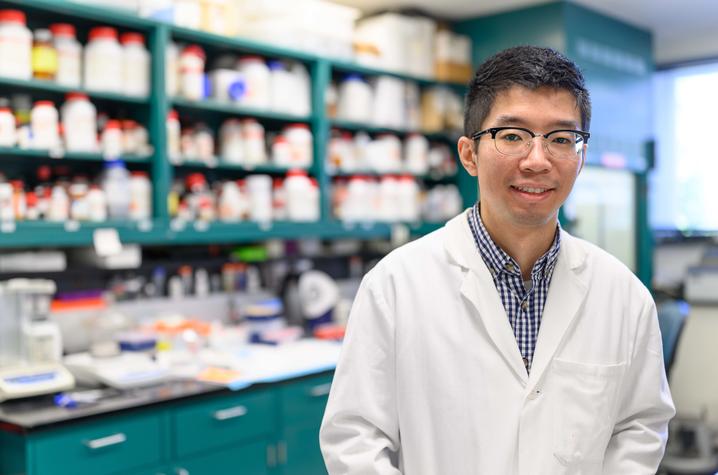
For about a week, UK chemistry doctoral student Yueming “Ronnie” Wu felt a little “off” — some stomach pains, a little constipation. Nothing too severe, and nothing necessarily out of the ordinary. With Memorial Day coming up, the Sanders-Brown Center on Aging researcher made plans to visit his girlfriend and her family for the long weekend. But that Thursday prior, his mild discomfort rapidly turned into full-blown illness.
“I began to throw up for two days, pretty much nonstop,” he said. “At the beginning, I thought it was just IBS (irritable bowel syndrome), so I just went to see the doctor at the emergency department, and they did a couple of tests and an ultrasound.”
In UK Chandler Hospital’s Emergency Department, Wu was first seen by Dr. Andrew Bernard, UK division chief of acute care surgery and trauma and professor of surgery in the UK College of Medicine. Bernard immediately ordered tests to rule out common health issues, like gallstones or indigestion.
“He didn’t really fit the model for gallbladder trouble — young, healthy guy with bloating and some belly pain,” Bernard said. “And we knew it was a possibility, but we certainly weren’t thinking it was cancer.”
Wu’s pain worsened and his abdomen became distended, swelling to the point where he describes pressing his hand against it like “pushing against a wall.” Further testing showed a narrowing in the colon, Bernard says, and the decision to take Wu to surgery was made. Bernard and Warriner met with Wu late in the afternoon to tell him he would be going into surgery that evening.
Warriner, who was covering the trauma night shift, took Wu into an operating room around 8 p.m. and worked on him late into the night. When Bernard assumed care early the next morning, he and his team were the ones to deliver the bad news: cancer. A lot of it, and far too much to be able to remove it all with surgery.
“My first thought is, ‘I don’t believe it,’” Wu said. “There’s no way. I know that type of cancer targets the demographic over 50, 60, and nobody thought it would happen at this age.”
But there was some good news, too — one of the benefits of being at an academic medical center like UK HealthCare is having access to complex, specialized care that’s not offered at every hospital, says Bernard. With the UK Markey Cancer Center literally in the next building over, Wu could meet with his oncology team and start on a treatment plan right away.
*****
After recovering from his emergency surgery, Wu began treatment with Markey medical oncologist Dr. Zhonglin Hao and hematology/oncology fellow Dr. Janeesh Veedu. Veedu’s three-year long fellowship began in July 2020, and Wu was one of his first patients.
“He was a young guy with no significant past medical history, but who was just diagnosed with stage IV metastatic colon cancer,” Veedu said. “So when I met him, he was in that stage where he was shocked by the diagnosis, and anxious about what we’re going to do and what his future is going to be.”
Though colorectal cancer is often considered a disease of the older population, the number of cases happening in people younger than 50 has risen sharply in the past 30 years. Hao and Veedu estimate that nowadays, roughly 12% of diagnosed colorectal cancers occur in people under the age of 50. Hao, a professor in the UK College of Medicine’s Department of Internal Medicine, has already been studying this trend, looking specifically at genetic alternations and tumor levels of young colorectal cancer patients.
Last year, the unexpected death of 43-year-old actor Chadwick Boseman from the disease shed some light on this unfortunate trend, and Hao says there should be more awareness of the potential of this disease in the younger population.
“People need to be aware that there is an increase in younger patients, and that slope is pretty steep — it’s a nearly two-fold increase since the early 1990s,” Hao said. “We shouldn’t keep thinking, ‘Oh, this cancer is a disease of the elderly.’ That is not right.”
Many early onset colorectal cancers are caused by two main mutations — Lynch syndrome and a mutation of the adenomatous polyposis coli (APC) gene — but genetic testing of Wu’s tumor showed neither of these. It did, however, show a mutation in TP53 — another tumor suppressor — in his colorectal cancer.
Hao and Veedu chose a variety of chemotherapies to target Wu’s disease: oxaliplatin, a powerful chemotherapy infusion that targets metastatic colorectal cancer; capecitabine, an oral chemotherapy that prevents cells from dividing/spreading; and panitumumab, a monoclonal antibody therapy also given intravenously. For six months, Wu received biweekly chemotherapy infusions of oxaliplatin and panitumumab and took the capecitabine pills every other week. Hao and Veedu monitored him closely for signs of toxicity, which can happen in potent chemotherapy regimens.
“Some of those months, I was doing labs on him every week,” Veedu said. “I was keeping close tabs on his numbers.”
At UK, Wu works in a lab at Sanders-Brown, researching potential ways to diagnose concussions earlier in athletes. As a scientist himself, he had a better technical understanding of what was going on in his body than the average patient might, and he was determined to keep himself educated about every aspect of his treatment plan.
“Most people will not do this, but when doctors introduced me to a type of treatment, I go home and go to the website, looking for the research papers to see what they do,” Wu said. “That's because with what my major is, I just naturally want to know how it works … knowing this makes me feel a little more comfortable.”
During the course of his treatment, Wu’s chemotherapy dose was reduced twice to help ease his side effects — in addition to feeling nauseous and tired, he began experiencing numbness in his fingers, a condition known as neuropathy. In cases like this, oncologists have to weigh the benefits of the drug against the negative effects and make a personalized decision about what’s best for each individual patient.
“Everyone responds to treatment differently. We have to monitor drug toxicity carefully in addition to response during treatment,” Hao said. “He was able to complete the full six months of marathon treatment with dose adjustment.”
Halfway through his chemotherapy schedule, Wu had a follow-up CAT scan and a colonoscopy. It was a major checkpoint in his cancer treatment journey.
“The thing I feared most is the first half of treatment, because the oncologists said, ‘We don’t know if the treatments will work or not,’” Wu said. “But after three months, they said that the treatment had been working well, and a lot of the tumor had been downsized. I said, ‘That’s the best news I’ve heard in a while.’”
And that news led him to meet the team of doctors who would take him on to the next phase of his care — a second major surgery to try to fully eliminate the cancer from his body.
*****
In October 2020, Wu met with Markey surgeons Dr. Sandra Beck and Dr. Prakash Pandalai to work out the next potential steps in his treatment plan.
“We met in the clinic, and we discussed this aggressive, radical surgery that he may or may not be a candidate for,” said Pandalai, assistant professor in the UK Department of Surgery. “Ronnie is a super smart guy, and he asked a lot of really smart questions. We bonded over the fact that he was critically thinking about how all this stuff was going to impact him.”
The “aggressive” treatment in question was cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy, commonly known as HIPEC. During this procedure, the surgery team first cuts out any sites of remaining visible cancer within the abdominal cavity. Once that step is complete, HIPEC begins: two catheters are placed in the abdomen to create a circuit with a machine designed to heat the chemotherapy in the abdomen to 103 degrees. One catheter pumps the heated chemotherapy into the abdominal cavity, while the second catheter brings it back into the machine. This circuit can run anywhere from 30 to 90 minutes depending on the type of chemotherapy used. In essence, it “washes” any remaining microscopic disease with the hot chemotherapy, with the goal of killing any lingering cancer cells.
“It’s highly effective at killing the cells we cannot see,” Pandalai said. “This is a treatment that’s not offered in many places, and we specialize in it.”
The goal of chemotherapy prior to CRS-HIPEC is to shrink as much of the tumor as possible, making it easier for the surgeons to then try to fully eliminate the disease. Though his six-month course of chemotherapy was difficult, Wu had an excellent response to the drugs, which thrilled his health care team and vastly improved his chances of a good surgical outcome. In late February, Wu underwent the lengthy CRS-HIPEC procedure with Beck leading the surgical resection and Pandalai in charge of the HIPEC portion.
Though the team uses imaging to prepare themselves for what they’ll find during the surgery, Pandalai says unexpected issues can happen. In Ronnie’s case, they were cautiously optimistic going into the CRS-HIPEC procedure.
“What you see on the imaging sometimes does not correlate to what you see inside the abdominal cavity,” he said. “In Ronnie’s case, you could see an amazing response to the tumor from the chemotherapy. So we were pretty optimistic from the beginning, and he did great. And when we got the results back after the surgery, it was just a home run.”
*****
Talk to any of the UK HealthCare physicians who have had a hand in treating Ronnie Wu over the past year, and they’ll tell you the same thing: he was a joy and a privilege to care for. Once the initial shock of his diagnosis had passed, it was clear that Wu became fully empowered in being a part of his own treatment team.
“I felt a real connection with him; I felt a lot of trust,” Bernard said. “Every subsequent visit he had with me, he was more energetic, optimistic and committed. I don’t remember him uttering a single time, ‘Poor me.’ There was none of that. He was an amazing guy.”
“As a patient, he was always very calm, he listened to us, he did everything we told him,” Veedu said. “He always asked the most important questions and always respected our decisions, and actually, he helped us guide his care. He’s one of those patients you’d like to have.”
“He is a fighter,” Pandalai said. “He was really scared when he first got diagnosed, but through his internal strength, he took control of the things that he could control — we talked about staying positive, nutrition, exercising as much as he felt like he could. These are all really important during treatments because your body has to heal from the chemotherapy and surgery. He was a model patient.”
Though Wu had moved on from their care, the emergency surgery team remained invested in his case. Warriner recalls how he would get updates on Wu’s treatment from resident physicians on the surgery team.
“They did his operation, gave him his chemotherapy, and then called me, ecstatic, to tell me that his pathology was negative,” Warriner said. “I just think that speaks to the benefit of being in a place like this, where you’ve got all these teams who support each other … it’s respect for another surgeon and for another team that has cared for him and was involved in making this diagnosis.”
Wu’s strength throughout the process is even more impressive against the backdrop of 2020 — due to the pandemic, he was unable to see his family in China, who he normally visits once a year. His chemotherapy treatment also meant he was at a higher risk for contracting and developing complications from COVID-19.
“The doctors said, ‘Your immune system is very weak, so don’t take any risks — just stay home and wash your hands a lot,’” Wu said. “I tried to avoid human contact as much as possible.”
Wu remained in isolation for much of the year, only going out for his medical appointments and the occasional trip to his lab or the grocery store pickup. He credits his roommate, UK College of Law graduate Zachary Holt, for helping him get through the past year — taking him to appointments, cooking meals for him, and even reviewing his medical paperwork.
“He helped me get food, he cooks, he was doing all the things,” Wu said. “Since he is an attorney, he reviewed a lot of the medical documents and legal paperwork. I don’t know what I would have done without somebody reviewing all that. My life would have been a whole lot more difficult without him.”
*****
Right now, Wu’s prognosis is good — after the successful CRS-HIPEC procedure, he is now considered NED — no evidence of disease. This means that testing currently cannot detect any cancer cells in Wu’s body. He will continue to receive scans on a regular basis to look for any recurrence, and Hao has added a new, even more precise way to monitor Wu: a new blood test called the Signatera QNS test. Also known as a circulating tumor DNA (or ctDNA) test, it looks for substances in the blood that colorectal cancer may produce — and would find this warning sign much earlier than a scan.
But for now, Wu is looking forward to getting back to a post-COVID, post-treatment life. He recently returned to full-time work in the lab and says he’s just taking things a day at a time. He decided to share his story to raise awareness of colorectal cancer in younger people, with the hope that his story helps someone in the future. And he has some optimistic advice for patients who find themselves in a similar situation.
“I would tell them, ‘Don’t freak out,’” Wu said. “Cancer treatment has advanced a lot in the past 5-10 years. Trust your doctors; they know what they are doing. Believe in the technology, medicine and the science.”
Spoken like a true scientist.