Zwischenberger and Wang receive FDA approval and Patent for Double Lumen Cannula
In their quest for perfecting the artificial lung, Department of Surgery Chairman Joseph B. Zwischenberger, MD and Director of the Artificial Organ Laboratory Dongfang Wang, MD, PhD have patented and received FDA approval of a new device which greatly improves the oxygenation of blood for patients who suffer from severe lung failure. The device, a two-channel catheter (in scientific terms, double lumen cannula or DLC) expands the potential application of extracorporeal membrane oxygenation or ECMO.
For thirty years, ECMO has been the primary treatment for adults with acute respiratory distress syndrome and end stage chronic lung disease. With these pathologies, the lungs are unable to infuse oxygen into the blood and expire carbon dioxide. Approximately 425,000 people in the United States are affected annually and the mortality rate is just below 40 percent.
With ECMO, a drainage cannula is introduced to the superior vena cava, where carbon dioxide needs to be expelled, and an infusion cannula is introduced to the aorta, where oxygen is circulated into the blood system. Blood is drained through the drainage cannula to a pump and an oxygenator. The oxygenated blood is returned to the body through the infusion cannula into the aorta. The ECMO procedure is bulky, complicated, labor intensive, invasive to the body, and inherently problematic. Cannulation of the major arteries is traumatic and can lead to ligation, occlusion of the major arteries, massive bleeding, stroke or amputation. It may also lead to cardiac stun syndrome since the oxygenated blood does not go through the heart. Another ECMO technique avoids major arterial damage by cannulating veins. Its disadvantages include insufficient venous blood drainage, insufficient oxygenation and undesirable blood recirculation.
Drs. Zwischenberger and Wang have investigated and/or tested approximately five alternative gas exchange techniques to achieve oxygen infusion/CO2 removal, but either the results are limited or the surgery required is too complex for clinical applicability. Their ultimate goal is to develop a minimally invasive, ambulatory paracorporeal artificial lung.
Such was the state-of- the-art of single lumen cannula procedures for adults. Until now, the double lumen cannula with two internal channels, for drainage and infusion respectively, has been successfully used in conjunction with ECMO for neonates and small children. However this device is insufficient for large children and there is no DLC for adults.
Designed to achieve total gas exchange for adults, the cannula is a significant step in this direction. “The double lumen cannula is simpler, but ten times more efficient,” said Dr. Zwischenberger.
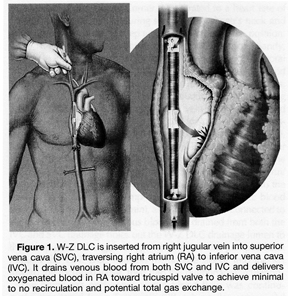
Teaming up with Avalon Laboratories Inc. in California, the Avalon Elite™ Bi-Caval Double Lumen Catheter is a high performance device that accomplishes total gas exchange for patients of all sizes with lung disease. The device is inserted into the right jugular vein traversing the superior vena cava and the inferior vena cava. There is minimal recirculation because of the positioning of drainage/infusion lumens and the ultra thin plastic membrane achieves minimal blood resistance. A significantly less traumatic “introducer” for easy insertion is fabricated from the collapsed infusion lumen, allowing it to be tapered. The Avalon Elite™ is made primarily of a polyurethane copolymer that combines the biostability of silicone with the strength and durability of polyurethane. To address kinking and maintain structural integrity, there is a stainless steel wire coil (0.1mm) reinforcement.
“The material is similar to a balloon and its construction allows it to assume the correct shape and function at a recirculation rate of twenty percent,” said Dr. Zwischenberger. He added, “Since FDA approval, Avalon has been unable to keep up with demand for the double lumen cannula.”
The DLC is manufactured and offered by Avalon Laboratories in seven different sizes. This new invention enhances the artificial lung’s gas exchange performance and it will help patients who are either waiting for a lung transplant or need temporary pulmonary support for damaged lungs. We send hearty congratulations to all involved.