Recent Faculty Publication: Cilostazol Attenuates Angiotensin II–Induced Abdominal Aortic Aneurysms but Not Atherosclerosis in Apolipoprotein E–Deficient Mice
Abstract
Objective—
Abdominal aortic aneurysm (AAA) is a permanent dilation of the abdominal aorta associated with rupture, which frequently results in fatal consequences. AAA tissue is commonly characterized by localized structural deterioration accompanied with inflammation and profound accumulation of leukocytes, although the specific function of these cells is unknown. Cilostazol, a phosphodiesterase III inhibitor, is commonly used for patients with peripheral vascular disease or stroke because of its anti-platelet aggregation effect and anti-inflammatory effect, which is vasoprotective effect. In this study, we evaluated the effects of cilostazol on angiotensin II–induced AAA formation.
Approach and Results—
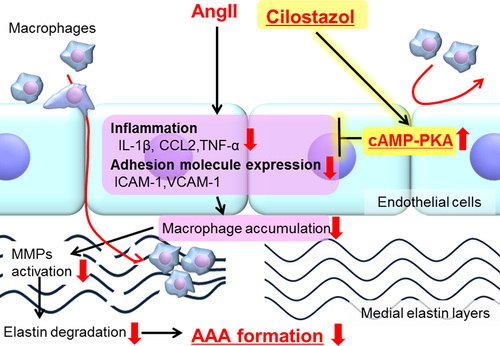
Male apolipoprotein E–deficient mice were fed either normal diet or a diet containing cilostazol (0.1% wt/wt). After 1 week of diet consumption, mice were infused with angiotensin II (1000 ng/kg per minute) for 4 weeks. Angiotensin II infusion increased maximal diameters of abdominal aortas, whereas cilostazol administration significantly attenuated dilatation of abdominal aortas, thereby, reducing AAA incidence. Cilostazol also reduced macrophage accumulation, matrix metalloproteinases activation, and inflammatory gene expression in the aortic media. In cultured vascular endothelial cells, cilostazol reduced expression of inflammatory cytokines and adhesive molecules through activation of the cAMP–PKA (protein kinase A) pathway.
Conclusions—
Cilostazol attenuated angiotensin II–induced AAA formation by its anti-inflammatory effect through phosphodiesterase III inhibition in the aortic wall. Cilostazol may be a promising new therapeutic option for AAAs.
Link to full article or see attached PDF
Saha Cardiovascular Research Center contributors, Drs. Venkat Subramanian and Alan Daugherty
Ryoko Umebayashi , Haruhito A. Uchida , Yuki Kakio , Venkateswaran Subramanian , Alan Daugherty , and Jun Wada